How do children get pneumonia?
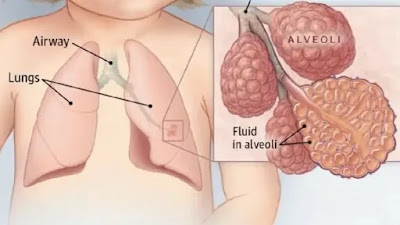
Children can get pneumonia through various means, and the most common cause is infection with bacteria, viruses, or other microorganisms. The infection typically enters the lungs, causing inflammation of the air sacs and leading to the development of pneumonia. Here are some common ways children can contract pneumonia: Bacterial Infections: Bacteria such as Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus can cause bacterial pneumonia. These bacteria can be spread through respiratory droplets when an infected person coughs or sneezes. Viral Infections: Viruses, including respiratory syncytial virus (RSV), influenza (flu), and adenovirus, are common causes of viral pneumonia. Viruses can be transmitted through respiratory secretions or by touching surfaces contaminated with the virus. Aspiration: Inhaling foreign objects, such as food, liquids, or vomit, can lead to aspiration pneumonia. This is more common in young children who may not have fully developed